Patient Identification: Each page in the medical record must contain the patient name or identification number. 3. Personal/Biographical Data: Personal and biographical data must be noted. This may include address, employer, date of birth, sex, marital status, and home/work telephone numbers.
What is required in a medical note?
The medical record must include Member identification, biographical data, emergency contact information, and informed consents.
What is considered medical documentation?
Typically, medical documentation consists of operative notes, progress notes, physician orders, physician certification, physical therapy notes, ER records, or other notes and/or written documents; it may include ECG/EKG, tracings, images, X-rays, videotapes and other media. …
What is a medical chart note?
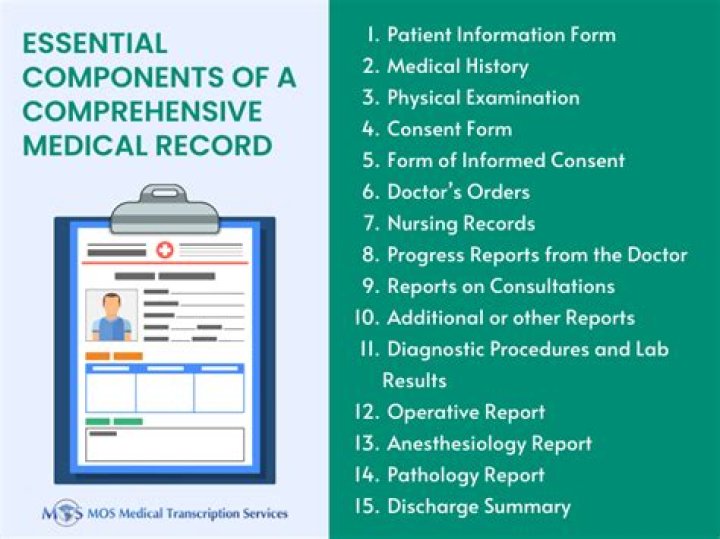
A medical chart is a complete record of a patient’s key clinical data and medical history, such as demographics, vital signs, diagnoses, medications, treatment plans, progress notes, problems, immunization dates, allergies, radiology images, and laboratory and test results.
What are examples of medical documents?
Tweet it!
- PIL. A PIL is a patient information leaflet you can find in any medicine bought at a pharmacy.
- Medical history record.
- Discharge Summary.
- Medical test.
- Mental Status Examination.
- Operative Report.
What is medical record documentation?
A patient’s medical record is the historical account of the patient/provider encounter and serves as a legal document for use in legal proceedings. Good healthcare decision making is dependent upon a provider’s ability to retrieve accurate and complete facts from the patient’s record.
How do you write a medical chart?
9 Tips for Writing Rock-Solid Medical Charts
- Keep it legible and professional.
- Beware of EMR laziness.
- It’s all about cause and effect.
- Stop procrastinating.
- Get consent and document it.
- Be complete and specific.
- Document refusal of care and noncompliance.
- Include follow-up instructions.
What are documentation Guidelines?
Documentation Guidelines. A comprehensive diagnostic report (e.g. MFE or ETR). Where appropriate, summary and data from specific test results should be attached. A learning disability assessment should include (a) a measure of cognitive aptitude (preferably normed for adults) and (b) a measure of achievement in reading, math and/or written language.
What is the purpose of medical record documentation?
Medical Records and Documentation Standards. The purpose of complete and accurate patient record documentation is to foster quality and continuity of care. It creates a means of communication between providers and between providers and members about health status, preventive health services, treatment, planning, and delivery of care.
What is proper health record documentation?
The medical record is the primary tool for documenting the care provided to a patient, and for communicating among other healthcare providers about that care. Proper documentation in the medical record—which is a legal document—is an essential component of quality patient care and effective risk management.
What is a physician documentation?
A term relating to a patient care or medical record. Typically, medical documentation consists of operative notes, progress notes, physician orders, physician certification, physical therapy notes, ER records, or other notes and/or written documents; it may include ECG /EKG, tracings, images, X-rays, videotapes and other media.