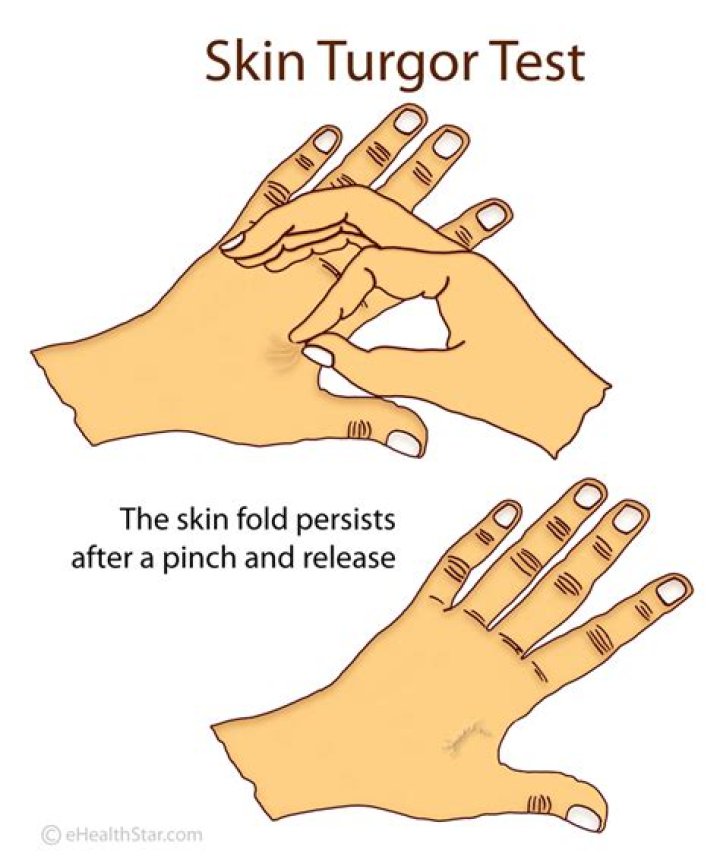
They main way to test skin turgor is to lightly pinch your skin, usually on your arm or abdomen. If it takes longer than usual for the skin to bounce back, it could be a sign of dehydration.
How do you document skin turgor in nursing assessment?
To check for skin turgor, gently grasp skin on the patient’s lower arm between two fingers so that it is tented upwards, and then release. Skin with normal turgor snaps rapidly back to its normal position, but skin with poor turgor takes additional time to return to its normal position.
What is a normal skin assessment?
A skin assessment should include an actual observation of the entire body surface, including all wounds*, inspection of hair, nails, skin folds and web spaces on hands and feet, systematically from head to toe.
How do you evaluate skin turgor?
To check for skin turgor, the health care provider grasps the skin between two fingers so that it is tented up. Commonly on the lower arm or abdomen is checked. The skin is held for a few seconds then released. Skin with normal turgor snaps rapidly back to its normal position.
How do you describe normal skin?
Normal Skin Type Not too dry and not too oily, normal skin has: No or few imperfections. No severe sensitivity. Barely visible pores.
What is skin turgor and how is it assessed?
The assessment of skin turgor is used clinically to determine the extent of dehydration, or fluid loss, in the body. The measurement is done by pinching up a portion of skin (often on the back of the hand) between two fingers so that it is raised for a few seconds.
How do you inspect and palpate skin?
Inspect and palpate skin for the following:
- Color: Contrast with color of mucous membrane.
- Texture.
- Turgor: Lift a fold of skin and note the ease with which it moves (mobility) and the speed with which it returns into place.
- Moisture.
- Pigmentation.
- Lesions.
- Hair distribution.
- Warmth: Feel with back of your hand.